Mirar esta página en español HomeJournal ContentsIssue Contents
Volume 12 Number 1
©The Author(s) 2010
Confronting the Baby Blues: A Social Constructivist Reflects on Time Spent in a Behaviorist Infant Classroom
Abstract
This reflective essay describes the author’s experiences as an observer in a behaviorist infant classroom. The author developed four categories of practice to describe what happened in the behaviorist infant room: (1) curricular focus on training typically developing infants to meet typical developmental milestones, (2) the use of highly structured play by staff as the means for meeting their training goals for the babies, (3) particular uses of language by staff in the behaviorist classroom, and (4) ways in which the staff’s adherence to core beliefs in behaviorism led to a lack of recognition of infants’ individual expressions of needs and wants. The article concludes with the author’s reflections on researchers’ ethical responsibilities when faced with an environment that they consider inappropriate and potentially harmful to children.
Eyes (and Ears) Opened by a New Experience
It was my privilege and delight to spend several months of 2009 learning, playing, laughing, and participating in the activities of dozens of infants and their caregivers in several different programs throughout the midwestern United States. I conducted a study of what it is like to be an infant who spends all day, every day, in high-quality child care. To do this, I spent a minimum of 2 weeks in each of several infant classrooms with babies, ages 3 to 18 months.
I had selected sites in laboratory schools or university-affiliated programs that had reputations for excellence in their communities and for which there was evidence that the caregivers engaged in the field’s “best,” “recommended,” or research-based practices with infants. The first three rooms in which I conducted my study aligned closely in terms of philosophy with the National Association for the Education of Young Children’s developmentally appropriate practices for birth to 3-year-olds (Copple & Bredekamp, 2009; McMullen, 1999). For example, each of these three rooms practiced continuity of care and primary caregiving.1 Although guided by a common philosophy, the caregivers in these infant rooms implemented curriculum in ways that made each room unique. These three rooms had in common a reliance on “relationship-based” principles (McMullen & Dixon, 2009). Thus, I will present them as a composite, referring to them collectively as the “relationship-based rooms” throughout the remainder of this article.
My criteria for identifying and selecting sites that were high quality worked well for those first infant sites that I visited. Based on this success, I entered my fourth infant room excited to meet a new group of babies and caregivers. Like the other programs, this one was in a lab school program affiliated with a major university. Program materials described it as “research-based,” “developmental,” and “appropriate.” It had a waiting list of parents eager to enroll their infants and a strong reputation in the community for being a “good place” to bring one’s children.
Within the first moments of my first day in this new classroom, however, my excitement dissolved into confusion. An excerpt from my journal from that day provides a glimpse of my initial experience:
Three minutes of solid, non-stop wailing, screaming…now four minutes. With each passing second, I feel the tension in my body grow. My head is pounding, my mouth is dry. I feel almost panicky and desperate to do something, to spring into action. Yet, I don’t; I sit, rooted to the floor, silent, painfully watching and listening to Baby Wendy, 3 months old, as she lies on the floor screaming one of those “I’m in distress! Do something NOW!” cries. But I can’t or I don’t. I’ve been told explicitly by the staff not to interfere, not just because I am a researcher, an outsider in this room, a guest, but because they don’t believe in picking up crying babies! They don’t pick them up, they say, until they stop crying on their own for 2 to 3 minutes. To do otherwise is to reinforce negative, unwanted behavior. I’m devastated and near tears myself; I hate myself for my own cowardice at not taking a stand on behalf of this child. (Journal Entry, Day 1)
In this classroom, I was faced with an environment and practices with infants that were not only foreign to me but that made me uncomfortable. I found the practice of not comforting or attending to crying babies disturbing and so antithetical to everything that I believe that I debated about even returning to the classroom. The final words that I recorded in my field notes that first evening were, “I feel heartsick.”
But, ultimately, I decided to go back a second day, and then again, and again. I had something to learn here, I felt, but wasn’t sure at first what it was. I needed to understand what was happening here, and to do so, I would have to try to look beyond the crying. Recognizing that this site was an outlier in my study, I tried to reframe my research questions as I reflected that first evening. Without changing my observation and interview techniques or data collection methods, I now decided to seek to understand, “What do the people in this setting believe and understand about infants and the care and education of infants?”
Unwittingly, I had stumbled upon a behaviorist infant classroom. The program and its staff based all assumptions about teaching, learning, and child development upon behavioral learning theories. I had studied behaviorism as a theoretical construct, and I have always believed it has some usefulness in animal training or when applied in limited ways to changing discrete human behaviors. But I had not heard of using behaviorist principles with groups of typically developing children—babies!—as the basis upon which to build and implement curriculum.
I spent 2 weeks in this room, along with eight babies, ages 3 to 12 months old. The experience opened my eyes—and ears—and has created a profound and lasting memory of my time in this classroom. I offer this reflective essay, not as a report of my research, but in part to process my own memories and to share my thoughts with others about the time I spent there.
I make no effort to hide how I feel about behaviorism with infants; my bias is obvious. In terms of philosophy, I am primarily a social constructivist who is guided by caring and social justice perspectives. In short, my scholarship, teaching, and service are shaped by theoretical perspectives largely influenced by the following: Lev Vygotsky’s (1962, 1978) work examining social and cultural influences on development, Nel Noddings’ (2003) ethic of caring and fundamental concern for how human beings treat one another, John Rawl’s (1999) conception that justice and social values (such as liberty, happiness, etc.) should be fairly accessible to all, and Kenneth Strike’s (1999) ideas of the complex interplay of caring and justice perspectives in the decisions we make that impact people (see also Lash & McMullen, 2008; Apple & McMullen, 2007). I hope that what I describe about my experience may prompt some interesting and meaningful discussion among readers in their own communities of practice, whatever their perspectives.
Behaviorist Practices with Infants Come into Focus
A major assumption of behaviorism is that the learner is passive; external stimuli and reinforcement of responses determine whether one learns or performs any given action. This belief was in full play in the behaviorist room, as I will now refer to it, where the staff carefully planned systems of positive and negative reinforcements, praise and rewards meant to increase or decrease the likelihood that babies would learn specific behaviors. John B. Watson (1878-1958) popularized behaviorism and applied it to infants and principles of child rearing, famously claiming:
Give me a dozen healthy infants, well-formed, and my own specified world to bring them up in and I’ll guarantee to take any one at random and train him to become any type of specialist I might select—doctor, lawyer, artist, merchant-chief and, yes, even beggar-man and thief, regardless of his talents, penchants, tendencies, abilities, vocations, and race of his ancestors. (Watson, 1930, p. 82)
As a mother of three, a former infant caregiver, and a social constructivist, I cannot accept the notion of the totally passive infant. I see babies as individuals who are full participants in the experiences of their lives—fully communicative human beings with agency, who seek, build, and maintain relationships that help them grow, develop, and learn about life and love, about caring and fairness, and about all the good and bad that the world has to offer, in mutuality with their relationship partners. Just as foreign to me is the idea that adults “teach” typically developing, healthy babies to master motor control of their bodies. I see infants wiggling and squirming, kicking and grabbing, reaching and moving, exploring every corner of their play spaces, learning through their own activity and, over time, growing stronger and more able to make their bodies respond to achieve their goals.
In trying to understand and communicate to others the essence of what made the behaviorist infant room unique, I have settled on four overarching sets of practices. I believe that discussing these categories of practice together will allow readers to see what happened in the behaviorist room during my observations and will highlight how it differed from generally recognized recommended practices with infants in the field today. The four categories are
- curricular focus on training typically developing infants to meet typical developmental milestones,
- the use of highly structured play by staff as the means for meeting their training goals for the babies,
- particular uses of language by staff in the behaviorist classroom, and
- ways in which the staff’s adherence to core beliefs in behaviorism led to a failure to recognize infants’ individual expressions of their needs and wants.
Focus on Training and Entertaining
The overall look and feel of the behaviorist room differed considerably from that of the relationship-based rooms and most child care rooms that I have visited in the United States. The room was long and narrow, with visible clutter stacked floor to ceiling along the length of one whole wall. It was dingy, and while the room and materials were probably clean, everything looked old, dirty, and worn. On my first day, I asked a supervisor to tell me who was responsible for room arrangement, including setting up and making physical changes and improvements. I was informed that the room had essentially looked the same way and had followed the same schedule for “years and years.” Its arrangement apparently had been determined well over a decade ago by “some professor”; no one had bothered to change it since then, nor apparently seen any reason to do so. While functional, the room was unattractive and uncomfortable for adults. In addition to the clutter and noise, there were lingering odors and no place for an adult to sit. I had to conclude that it was probably not a physically comfortable or pleasant environment for babies to be 8 hours a day, 5 days per week, either.
The curriculum in the behaviorist classroom was based upon scheduled trainings. Babies in this classroom were “taught” the basic milestones of child development—for example, rolling over, sitting, grasping, standing, creeping, and crawling—or so the caregivers seemed to believe. Every baby had several training goals that the staff worked on with them during each of the three shifts of the day. Training was rigorous and taken very seriously. Samples of some of the goals for four of the eight infants in the room are shown in Figure 1.

Figure 1. Chart of training goals for four infants.
Staff members worked on the goals with individual babies during scheduled play times, moving them into position, cajoling them, pleading with them, speaking to them in loud sing-song voices, gesturing, ordering them, and sometimes doing the tasks for them. If a baby accomplished the desired behavior on his or her own, the staff member would first verbally praise the child and then shout out to another adult in the room, for example, “Tammy pulled to hands and knees at 9:43 a.m. Record it.” Babies who accomplished a goal with assistance were also praised: “Good rolling, Tammy. That’s the way to roll!”
Babies who were not at that moment being trained were entertained until it was their turn for training or until another staff member came to get them to feed them, change them, or put them down for their scheduled nap. I refer to what they did as entertainment, because there was an intensity to it. Even though this was during play time, there was never a time that babies were just allowed to “be” or to make their own choices. Rather the staff members were always waving things in their faces, asking them to play with certain toys or to do specific activities, trying desperately to keep them busy, or trying to sing or make noise to distract them from crying. Staff activity and movement were constant and exhausting to watch.
I want to emphasize that these small infants were praised verbally during their trainings, but not physically. Just as no physical comfort could be offered to a crying baby, I saw little evidence of touch offered as a reward or reinforcement. For example:
Richie was praised, verbally and effusively, for stacking the blocks as requested during his training time by the staff. He smiled broadly and seemed very pleased and started to climb up on the staff member’s knees, but she gently but firmly pushed him away and said, “No; you know you cannot climb up on me.” I think he just wanted a hug or a little pat from her. (Journal Entry Day 6)
Families were expected to work on training goals at home as well. When Denny took what were purported to be his first two unassisted steps that the staff had seen, I asked, “Do you know if he has been walking at home yet?” A staff member responded, “I’m sure his parents are working on this at home. They work really hard on stuff.”
This conversation and others with staff members in the behaviorist room led me to conclude that they believed that adults were responsible for babies’ achieving skills defined by the training goals they set, which would otherwise be considered natural developmental milestones for typically developing infants. For example, I noted the following in my field journal:
When Billy’s older sister came with mom to pick him up today, she saw him pull himself up from hands and knees to a kneeling position in front of a shelf. “Wow! How did he learn to do that!?” she said. “Oh, we taught him that here,” said the staff member. (Journal Entry Day 3)
I hesitate to write about the staff in the behaviorist room as “caregivers.” I have always preferred this title, or the closely related term “care provider,” for the professional who works with very young children and their families. This preference is not because I discount the role that these individuals play as educators but rather because I value so highly the interpersonal, relationship-promoting components of their roles—the caring aspects. The adults that I observed in the behaviorist room could better be characterized as “trainers” or perhaps at times “entertainers” but not as givers of care. They seemed concerned with relating to the babies not as persons but as objects. That is why throughout this paper, I refer to those who worked in the behaviorist room as “staff” and those who worked in the relationship-based rooms as “caregivers.”
The staff and staffing patterns differed markedly between the two types of classrooms. In a typical day, the eight babies in the behaviorist room saw a minimum of eleven different adults across three different shifts who interacted with them as their “teachers.” None of the behaviorist classroom staff, including supervisors, were professionally trained in early childhood education or child development. The staffing was further complicated by the fact that staff during any given shift had specific assigned jobs that rotated every half hour throughout the shift, as follows: one would be in charge of feeding, one would oversee sleeping and “toileting,” and one would be assigned to manage the play and address training goals. Emphasis in the classroom seemed to be on shifting responsibilities evenly among the adults as frequently as possible, rather than on primary caregiving and relationship building.
In contrast, the relationship-based rooms that I visited each had three professionally educated and trained caregivers on staff, at least two of whom were present at any given time throughout the day. In each room, two of the three caregivers had at least a bachelor’s degree in early childhood education or child development; several had master’s degrees. The third member of the caregiving team in each relationship-based room had at least a CDA (Child Development Associate) credential but, more typically, an associate’s degree (two-year college degree). Numerous preservice student teachers, volunteers, and other adults tended to come in and out of the relationship-based classrooms regularly; these adults were always supervised by the professional caregivers and were never counted in adult:infant ratios.
Language Use during Infant Training
Language in the behaviorist room was purposeful in that it was used to achieve training goals, but it was rarely meaningful or interesting. The following sample, spoken by one staff member, was recorded during a 5-minute period as she sat on a floor mat with several babies during a play period:
“Good reaching! Good reaching out. Good reaching out for that.”
“What’s on Billy’s shirt? Billy, what is on your shirt?” (Staff member never followed through to identify the big number 2 on the shirt with the giraffe.)
“Let’s practice rolling.” (Staff member worked for a minute rolling a baby from stomach to side and back down again.) “Let’s roll. Good rolling, Lilly.”
“Nice job looking around.”
“Hi, Tammy. You’re facing all of your friends. I see you facing your friends. Good job looking at me now. Good looking.”
“Good mouthing, Andrea. You are good at mouthing.”
“Yah! Wow! You are so good! Good job, dude!”
“This is how we crawl, buddy…crawl, crawl, crawl.” (Staff member moves the knees and arms of a baby who is already up on his hands and knees forward across the floor two or three steps.) “Good crawling.”
“No matter which one you have, you want the one the other baby has.” (Staff member says, with exasperated sigh.)
“Wow! I am so impressed that you completed that roll. Good rolling.” (Staff member rolls a baby from stomach to back, stomach to back two times, then praises baby.)
“This one clicks when you turn it. Use it. Don’t use that one.” (Staff member takes toy from a baby who is examining it, apparently because it doesn’t make a sound, handing him one that makes noise.)
“Denny, you don’t need to be over there.” (Staff member moves Denny several feet away from a younger baby, although the two seemed to have been contentedly playing side-by-side with their own small toys.)
“Your turn to go potty.” (Staff members refer to diaper changing as “pottying” and “going potty.” They help all babies crawl or hold them by or under the arms to walk them to the diaper-changing area. Staff members told me that this is done so that the children learn to “go potty” independently.)
“Denny. Look. Look at this. You need to look at this.”
“Good job. Nice job.”
“Can you bang on it? Good banging! Can you shake it? Good shaking!”
“Do you see the window? Good looking at the window.”
“Good talking. And, good smiling, buddy!”
“That’s a purple turtle; say p-p-p-purple.” (Said to 7-month-old who seems to be gazing at a cartoonish turtle.)
“Reach in like this.” (Staff member moves baby’s arm into shape sorting bucket.) “Good job, Jenny. Look, Jenny has the yellow triangle! Yah, Jenny.” (Staff member holds her own hand around Jenny’s hand, clasps yellow plastic triangle, grabs triangle, and pulls it with Jenny’s hand from the from the bucket.)
“Show me stacking. I want you to stack 3. Show me stacking. More stacking.”
In short, the language use that I saw in the behaviorist room is not what I recommend when I suggest to parents and caregivers to “bathe babies in language.” Behaviorist staff members’ use of language could be described as a steady stream of chatter, mostly delivered in clipped, frenetic tones. They used praise frequently, as well as some direct commands, but real conversation was rare, and when it occurred, it was usually only among adults. These patterns of language use were quite different from what I experienced in the relationship-based rooms in my study. There, language flowed naturally as caregivers conversed with each other and communicated directly with babies. Although the babies in the behaviorist room were clearly exposed to lots of language—some of it directed at them—it was certainly not of a conversational, back-and-forth nature. On the rare occasions that staff members sang songs in the behaviorist room, the songs were adult oriented; a staff favorite was the university fight song.
Absurd Outcomes of Play as a Means to Adult Ends
Every minute in the behaviorist classroom was rigidly scheduled. The entire day was broken down into 15-minute increments, based upon a schedule of toys to be rotated and changed during each segment. A sample schedule is shown in Figure 2. Eating and diaper changes and, as much as possible, sleeping were also scheduled, seemingly arbitrarily. No matter what a baby happened to be doing at any given time or whether they needed it or not, if it was their time to eat, sleep, or be changed, it was done. In contrast, infants in the relationship-based rooms were fed when they were hungry, changed when their diapers needed changing, and put down to nap when they were sleepy. Their caregivers made adaptations when unexpected opportunities arose or unpredictable circumstances warranted; daily schedules seemed to function as flexible guidelines, giving structure and providing predictability and comfortable routine in the relationship-based rooms.
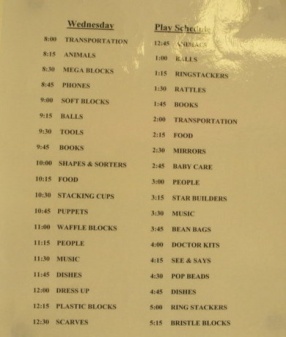
Figure 2. Toy rotation schedule.
Sample Toy Rotation Schedule for One Day
Wednesday Play Schedule
12:45 Animals
1:00 Balls
1:15 Ringstackers
1:30 Rattles
1:45 Books
2:00 Transportation
2:15 Food
2:30 Mirrors
2:45 Baby Care
3:00 People
3:15 Star Builders
3:30 Music
3:45 Bean Bags
4:00 Doctors Kits
4:15 See & Says
4:30 Pop Beads
4:45 Dishes
5:00 Ringstackers
5:15 Bristle Blocks
8:00 Transportation
8:15 Animals
8:30 Megablocks
8:45 Phones
9:00 Soft Blocks
9:15 Balls
9:30 Tools
9:45 Books
10:00 Shapes and Sorters
10:15 Food
10:30 Stacking Cups
10:45 Puppets
11:00 Waffle Blocks
11:15 People
11:30 Music
11:45 Dishes
12:00 Dress-up
12:15 Plastic Blocks
12:30 Scarves
In the behaviorist room, the physical positions of the non-mobile babies were also scheduled. Staff members would literally change these babies’ body positions at the same time as the toys, every 15 minutes, propping them first on one side then on the other, then on their backs, then their tummies, then in a device that assisted them in standing upright. This routine continued all day. No concern was shown for what the baby wanted or what positioning might be more advantageous for a given activity, or even whether or not the baby was comfortable. The staff did not appear to consider if a baby was able to get into or out of a position or device under his or her own power. The behaviorist dogma in this room led to the policy that every 15 minutes, non-mobile babies’ positions were to be changed.
I was informed that, like the classroom arrangement, the daily schedule of play and toy rotation, and the toys and books themselves, had remained essentially unchanged for many years. The adults carefully managed play time and play materials. Toys were stored in plastic bins, on long, tall shelves, to be accessed only by the staff. Figure 3 shows a section of the toy shelves with rows of plastic bins labeled with the category or type of toys within. Using a laminated schedule posted for each day of the week, staff members selected one new bin of toys every 15 minutes, placing the toys from that bin on a brightly colored plastic floor mat for the babies. After 15 minutes, the babies were moved to a second floor mat, on the other side of the room, where another bin of toys had been emptied, for them to look at or play with. The toys on the first mat were then picked up and put away in preparation for the next rotation. Fifteen minutes later, the babies were moved back again to the first floor mat, and so on. This toy rotation proceeded for the entire day, day after day, throughout my observations.

Figure 3. Toy shelves in the behaviorist classroom, showing plastic bins of toys.
Staff members told me that they scheduled the day this way so that the babies “would not get bored.” However, I often observed babies there who appeared bored and disengaged. They were given no choice of toys, and few of the toys provided were appropriate for their age group. The babies in the photograph in Figure 4, taken during a waffle block rotation, illustrate these two points. Readers may judge for themselves these babies’ level of engagement with the play materials. In addition to waffle blocks, toys in the behaviorist room included dishes and kitchen utensils, ring stackers, soft blocks, balls of many sizes, baby care thematic kit, musical instruments, toy phones, animals, plastic blocks, c-rings, mirrors, dress-up, scarves, shapes, little people, doctor kits, transportation, pop beads, puppets, rattles, toy food, star builders, books, bean bags, mega blocks, large blocks, bristle blocks, stacking cups, and plastic tools.

Figure 4. Babies during waffle block rotation.
Of the stories I could share related to play and its role in accomplishing adult goals, none was as striking to me as the anecdote below involving Babies Teddy and Tammy. Other babies in the room at this time were either asleep, being changed, or being fed:
It is the “Baby Care” toy rotation. The plastic “baby care” bin has several baby dolls, plastic bottles, rattles, blankets, baby clothes, etc. The contents of the bin lie in a pile on the play mat where the staff member sits cross-legged. Baby Tammy (4 months) is on her back right next to the staff member, screaming bloody murder, literally inches away, completely ignored. Howling. Red-faced. Baby Teddy (12 months) is crawling around the mat contentedly. The staff member dutifully tries to engage him with that 15 minutes required toy selection. “Oh, Teddy, look at the baby” (as she picks up a plastic baby doll from the pile of toys). “I think she’s crying…WAHHH WAHHH WAHHH. What do you think she needs?” Baby Teddy sits back on his bottom and looks at her. Staff rocks the plastic baby vigorously back and forth, talking gently and cooing to it. Meanwhile, the real Baby Tammy continues to SCREAM. Staff makes fake “WAHHH WAHHH WAHHH” crying noises again, pretending they are coming from the plastic baby. “Teddy, how can we help this poor baby? Should we try to wrap her in the blanket and give her a bottle? I wonder if she’s hungry.” The staff member wraps the doll up, and while Baby Teddy looks on, she rocks and “feeds” the bundled plastic baby, big exaggerated rocking movements on her lap back and forth, singing it a song. Real Baby Tammy continues to scream on her back inches away from the staff member. (Journal Entry, Day 9)
This interaction seemed absurd, considering what both Tammy and Teddy might have learned from this experience about life, love, caring, and relationships.
(In)Sensitive Responsiveness and Adult-Child Relationships
As one might surmise, the emotional climate of the behaviorist room was stressful—for me certainly, but I believe it was also for babies, for caregivers, and for parents. I observed some periods of calm and even fun in the behaviorist room; after all, how can there not be some fun with babies present? For far too many hours, however, the babies were bored, disengaged, or generally fussy; then there was the crying, punctuated far too frequently by infants screaming. The emotional tone in the behaviorist room contrasted sharply with the low-level, busy, peaceful hum of sound and activity that characterized the climate in the relationship-based rooms that I had visited previously.
A major difference that I observed between the behaviorist and relationship-based rooms was the lack in the former of what is generally considered a key aspect of infant caregiving—sensitive responsiveness on the part of the adults (McMullen, 1999). To be sensitively responsive, a caregiver needs to recognize the communication attempts of the babies in her life, to interpret their meaning accurately, and to respond appropriately in a timely manner. Caregivers can do this best, I believe, if they have developed relationships with the babies and thus recognize how they communicate their preferences, wants, and needs. Those of us who support this belief recognize crying as one of the primary ways that babies communicate. In the behaviorist room, however, infants’ cries were not valued as communication. No effort was made to understand them or to distinguish different cries; they were simply undesirable behaviors that needed to be extinguished. The staff in the behaviorist room worked on that goal diligently. The following vignette provides an example:
The staff member sits on the floor next to Baby Emma (3½ months) who is crying loudly. She turns, looks at her, and leans her body completely over Baby Emma’s, looks directly in her face. She says the baby’s name in a raised voice, “EMMA, EMMA.” And then…POUND POUND POUND…she bangs her hands loudly and vigorously on both sides of the play mat next to Emma’s ears. Again, POUND POUND POUND. “Look at me, Emma. LOOK AT ME!” Baby Emma screams. The staff member looks away, again. Another couple of minutes pass, now three. The staff member turns back again toward Baby Emma. This time she waves a rattle just a couple of inches above Baby Emma’s face. “Look, Emma. LOOK!” Baby Emma’s shrieks begin to abate, becoming deep, wrenching, breathy cries. Through her tears, Baby Emma opens her eyes and looks at the caregiver. “Good looking, Emma! You’re doing a very good job looking!” says the staff member, who then turns away again. Baby Emma sobs quietly but steadily. This goes on a couple more minutes. Finally, spent, Baby Emma stops crying and stares off into space. (Journal Entry, Day 7)
Sometimes one or more babies’ cries seemed to become sufficiently annoying that the staff in the behaviorist room simply could not ignore them. At such times, I saw the staff engage in a number of strategies to get the babies to stop crying, short of actually discerning what the babies wanted or needed. I observed several scenes such as that portrayed in the Baby Emma story. Staff attempted, sometimes with success, to startle, entertain, or distract babies to get them to stop crying. They employed various noises and sounds, using their own voices or nearby objects, toys, or surfaces. A couple of times I saw a staff member blow a puff of air into or over a baby’s face.
When I asked why they never picked up babies or held them, crying or otherwise, even to read to them, the supervisor informed me, “That is too easy.” Furthermore, I was told, they didn’t want babies to get used to being held or picked up whenever they wanted it.
As a consequence, I observed little physical contact between the adults and the babies. Parents, rather than being given advice about what their babies might be communicating with their cries, were asked to reinforce techniques at home to decrease or eliminate crying.
After a few days in the behaviorist room, I was ashamed to realize that I hardly noticed the crying any more. I had become numb to it—a survival response, I suppose. I observed that even the babies themselves did not seem to notice when a peer cried. In contrast, in the relationship-based rooms, crying from one baby typically attracted the attention of other babies and always elicited some kind of response from the caregivers. I likened my reaction to a time when I had lived next to well-used train tracks. After a few weeks of living there, even though I certainly heard the train as it roared by, I really didn’t attend to it anymore. When I made this connection—that I was ignoring the cries of these human babies the same way that I might a noisy train—it gave me pause.
First and foremost, I was concerned that my ability to ignore the babies’ cries meant that I was becoming callous and unconcerned about the babies. If this could happen to me, what did it mean for the babies in the room in terms of their own development as caring individuals? What lessons about caring did they learn when they were being conditioned to tune out the cries of their “friends?” What lessons were they learning about their own self-worth when they cried out in pain, hunger, or fear, or in an attempt to seek human warmth and affection, and were ignored?
Basically, social-emotional development did not seem to be a priority in the behaviorist room. Nothing was done to bring babies together to foster a sense of belonging to a community. Not only were one-on-one or small group peer interactions not encouraged, but I observed episodes when they were actively discouraged. Staff members expressed concern that older or bigger babies would harm younger, smaller ones if they got “too close.” In contrast, in the relationship-based rooms, the caregivers frequently created pairings or formed small groups of peers for various activities, staying as close as necessary to support play, and sitting on the floor close to the babies, all of which seemed to me to foster a sense of belonging to a community. Several times I heard caregivers in relationship-based rooms say variations of, “Gentle, please. Be gentle with your friends.” I also noted some friend preferences among babies in the relationship-based classrooms but not in the behaviorist room.
Revisiting and Reaffirming My Beliefs
Despite being haunted by a number of lingering images and lasting doubts about my time in this classroom, I think it is good that I went back after that first day in the behaviorist room and spent the full 2 weeks there as planned. I often urge my students to welcome opportunities in which they face some cognitive dissonance and are forced to question or revisit their long-held beliefs. I tell them that it is good to shake up old, dusty assumptions about how things are supposed to be. Yet when faced with such a challenge myself, I almost ran from it. I came to value this experience precisely because it exposed me to people with beliefs and practices in sharp contrast to the field’s widely accepted and my own deeply held understanding of best practices. It helped me reflect on and confirm what I believe in a way I never had before.
My experience in the behaviorist infant room convinced me more than ever before about the importance of nurturing and respecting the relationships that form between babies and caregiving adults. I hope that I will not forget these lessons and never take my own beliefs and philosophy about infant care and education for granted again. I also hope to help my students understand that what we teach them about relationship-based care is not “a no-brainer,” or “simply intuitive,” something “anyone would do,” as some of them have said to me.
My experience in the behaviorist room also allowed me to reflect upon what it means to be a researcher and an advocate; specifically, it has made me ponder how one can do both well at the same time. On the door of my office is an old worn bumper sticker that says, “I speak for babies.” I’ve stared at that sticker many times as I’ve reflected upon my experience in the behaviorist room. I reread our field’s Code of Ethics (NAEYC, 2005) seeking inspiration about how to negotiate the tangle of emotions and doubts that remain with me to this day. I did not speak up for the babies or for their parents or for the staff for that matter during my time in the behaviorist room—or if I did, I did so only weakly through questioning what I saw and explaining “what I was more familiar with” when anyone asked. I felt that it was not my place as an “outsider,” as a “researcher,” as a “guest.” I’m still left with questions, which I will pose to readers: What is or was my responsibility as a researcher in that room? What would you do under similar circumstances?
Consider this statement from Section I of the Code of Ethical Conduct Addressing Ethical Responsibilities to Children, Principle 1.1:
Above all, we shall not harm children. We shall not participate in practices that are emotionally damaging, physically harmful, disrespectful, degrading, dangerous, exploitative, or intimidating to children. This principle has precedence over all others in this Code. (NAEYC, 2005)
I accept that by doing nothing I participated in what I believe to be, at the very least, behaviors that were inappropriate and disrespectful toward infants. Was it harmful to them? I don’t know; whether harm was done may depend on the infant. I worry still about outcomes for infants who spend large amounts of time in environments in which social-emotional curriculum and prosocial skills are not valued (McMullen et al., 2009). In my opinion, the behaviorist environment did not contribute to their social-emotional growth or to their rights to be happy and enjoy their lives as productive, contributing members of the classroom. Now that is something to cry about.
Note
1. In infant-toddler care in the United States, a primary care system involves assigning a small group of children to one caregiver. Continuity of care refers to having infants remain with one caregiver or set of caregivers continuously from the time they are enrolled until they are 36 months old or leave the program.
References
Apple, Peggy, & McMullen, Mary Benson. (2007). Envisioning the impact of decisions made about early childhood professional development systems by different constituent groups. Contemporary Issues in Early Childhood Education, 8(3), 255-264.
Copple, Carol, & Bredekamp, Sue (Eds.). (2009). Developmentally appropriate practice in early childhood programs serving children from birth through age 8. Washington, DC: National Association for the Education of Young Children.
Lash, Marsha, & McMullen, Mary. (2008). The child care trilemma: How moral orientations influence the field. Contemporary Issues in Early Childhood Education, 9(1), 36-48.
McMullen, Mary Benson. (1999). Research in review: Achieving best practices in infant and toddler care and education. Young Children, 54(4), 69-76.
McMullen, Mary Benson; Addleman, Jennifer M.; Fulford, Amanda M.; Moore, Sarah L.; Mooney, Shari J.; Sisk, Samantha S.; & Zachariah, Jasmine. (2009). Learning to be me while coming to understand we: Encouraging prosocial babies in group settings. Young Children, 64(4), 20-28.
McMullen, Mary, & Dixon, Susan. (2009). In support of a relationship-based approach to practice with infants and toddlers in the United States. In Donna Berthelsen, Joanne Brownlee, & Eva Johansson (Eds.), Participatory learning and the early years: Research and pedagogy (pp. 109-128). London: Routledge.
National Association for the Education of Young Children. (2005). Code of ethical conduct and statement of commitment. Retrieved December 21, 2009, from http://frn.sdstate.edu/CodeofEthicsApril2005.pdf
Noddings, Nel. (2003). Caring: A feminine approach to ethics and moral education (2nd ed.). Berkeley: University of California Press.
Rawls, John. (1999). A theory of justice. Cambridge, MA: Harvard University Press.
Strike, Kenneth A. (1999). Justice, caring, and universality: In defense of moral pluralism. In Michael S. Katz, Nel Noddings, & Kenneth A. Strike (Eds.), Justice and caring: The search for common ground in education (pp. 21-37). New York: Teachers College Press.
Vygotsky, L. S. (1962). Thought and language. Cambridge, MA: MIT Press.
Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes. Cambridge, MA: Harvard University Press.
Watson, John B. (1930). Behaviorism. London: Kegan Paul, Trench, Trubner.
Author Information
Mary Benson McMullen, Ph.D., is Professor of Early Childhood Education and Associate Dean for Graduate Studies at the School of Education at Indiana University, Bloomington. She is a former infant, toddler, and preschool teacher and program administrator. Her research, teaching, and service focus on relationship-based practices with infants and toddlers, the connection between professional beliefs and practices, quality indicators in early childhood environments, and the professional development of early childhood practitioners in a variety of fields.
Mary Benson McMullen, Ph.D.
Department of Curriculum and Instruction
School of Education, Indiana University
201 North Rose Ave.
Bloomington, IN 47401
Email: mmcmulle@indiana.edu